Technical difficulties
I apologize...but right now I can't post new information due to the fact that the computer that I used to download pictures is down. Sorry for the incovenience.
Regards,
Luis
posted by luisbracero @ 6:49 PM
![]()
![]()
Blog dedicated to the Medical Technology Field plus personal experience along with my adventures here in Michigan.
I apologize...but right now I can't post new information due to the fact that the computer that I used to download pictures is down. Sorry for the incovenience.
posted by luisbracero @ 6:49 PM
![]()
![]()
Christmas is getting there and I received yesterday the gifts from my family....each one of them sent me a gift....but I guess from all the gifts that I received ..the one that I really like it was all the love on the postcards...I received a postcard in Spanglish(half spanish and half english)...and was hilarious....I missed so much my family, friends and specially my daughter. I asked Santa if he can bring me for christmas some company....but just a good one.....hope he bring me what I asked for christmas....
posted by luisbracero @ 10:19 PM
![]()
![]()
 Smudge Cell in a Patient with Chronic Lymphocytic Leukemia Immersion Oil 100x
Smudge Cell in a Patient with Chronic Lymphocytic Leukemia Immersion Oil 100x Gram positive cocci in chains in positive blood culture Streptococcus pneumoniae Immersion oil 100x
Gram positive cocci in chains in positive blood culture Streptococcus pneumoniae Immersion oil 100x Prolymphocyte in peripheral blood smear Immersion Oil 100x
Prolymphocyte in peripheral blood smear Immersion Oil 100x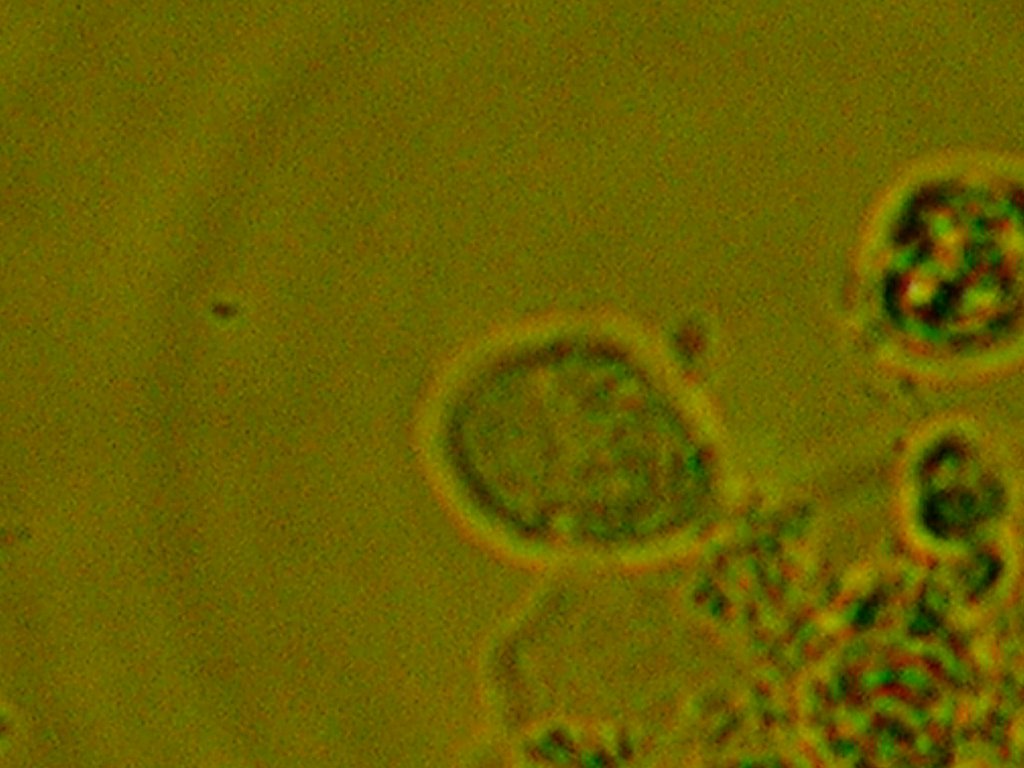 Trichomonas vaginalis in a Wet mount Immersion Oil 100x
Trichomonas vaginalis in a Wet mount Immersion Oil 100x Blast Cell in Peripheral Blood Smear Immersion Oil 100x
Blast Cell in Peripheral Blood Smear Immersion Oil 100x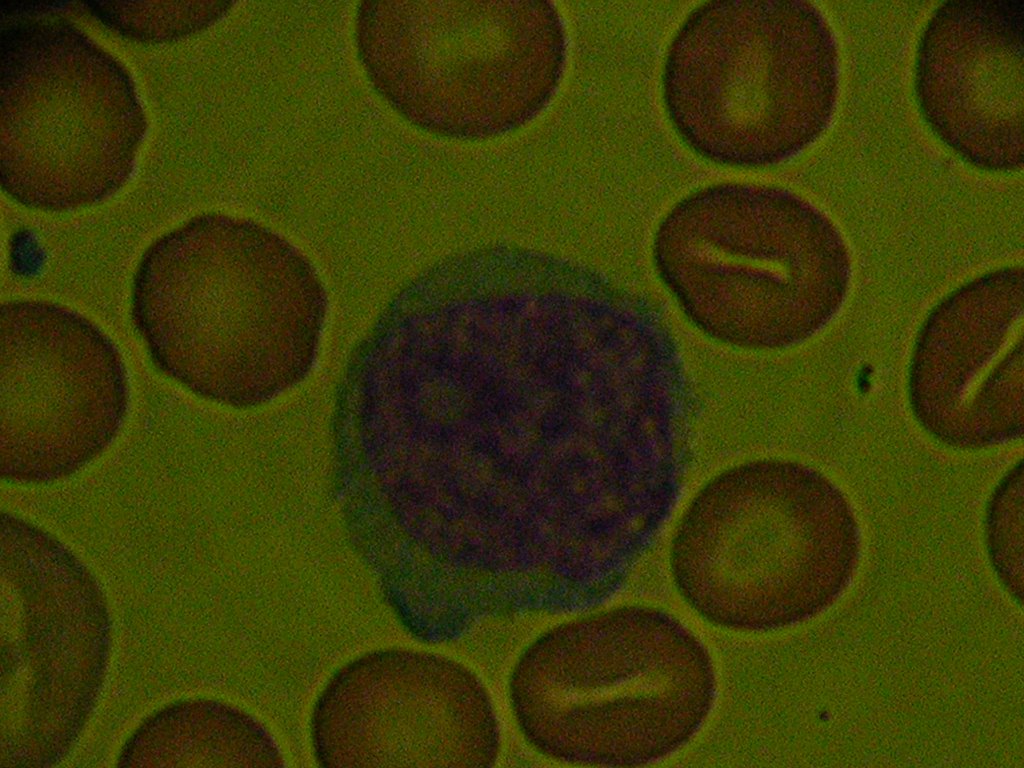 Blast Cell and Stomatocyte in Peripheral Blood Smear Immersion Oil 100x
Blast Cell and Stomatocyte in Peripheral Blood Smear Immersion Oil 100x
posted by luisbracero @ 7:49 AM
![]()
![]()
Sideroblastic Anemia is anemia associated with mithochondrial iron loading in erythroid precursors in the bone marrow and also associated with defective production of red blood cells. Causes of this type of anemia include:
posted by luisbracero @ 7:29 AM
![]()
![]()
Even with efforts by the US Goverment to combat this very common anemia still its prevalence. More common in women and childs than men. Iron deficiency anemia can occur from the following conditions; Nutritional deficiency, incomplete iron absorption, increase demand of iron or excessive loss of iron. Nutritional deficiency can occur if not enough iron is taken by dietary or from an imbalanced vegetarian diet. Incomplete iron absorbtion can occur in diseases like celiac disease, sprue, resection of the small vowel or absence of factors for the iron intake. Increase demand ocuur in childhood, pregnancy or increase period of blood regenaration. Excessive loss of iron can occur from chronic blood loss, heavy menstruation or abnormalities on the gastrointestinal tract. Laboratory findings in this type of anemia include hypochromic and microcytic anemia, Hemoglobin and hematocrit decreased, decreased MCV,MCH and MCHC, increase serum iron, increase tottal iron binding capacity, increase percentage of saturation and decreased ferritin ( iron storage). In this picture you can see a lymphocyte which is our reference about size. Usually the red cells are almost the same size of the nucleus of the lymphocyte.Also can be notice a bigger central pallor ( hypochromia).
 Iron Deficiency Anemia
Iron Deficiency Anemia
posted by luisbracero @ 11:50 PM
![]()
![]()
Chronic blood loss anemia can be related with heavy menstruation in women,urinary tract abnormalities and very often with disorders in the gastrointestinal tract. The blood loss is usually in small amounts for extended period of time. This blood loss does not disrupt the blood volume. At the beggining the anemia seen can be normochromic and normocytic until the iron storage is depleted. Once the iron storage is depleted can be seen hypochromic and microcytic anemia. White blood cell count is normal and platelets can be increased. A person with gastrointestinal bleeding can present a positive fecal blood test (occult blood in feces).
posted by luisbracero @ 11:34 PM
![]()
![]()
Acute blood loss anemias are related with severe injury, accidents or surgery.
posted by luisbracero @ 9:17 AM
![]()
![]()
 Poikilocitosis.
Poikilocitosis. Anisocytosis. 100x Immersion oil.
Anisocytosis. 100x Immersion oil. Hypochromia. 100x Immersion Oil
Hypochromia. 100x Immersion Oil
posted by luisbracero @ 11:42 PM
![]()
![]()
Anemia is something very common and is defined as the hemoglobin and or hematocrit below the lower limit within the 95% reference interval for age,sex and geographic location. From that at least 2.5% of individuals are classified as anemic. Anemias can be absolute or relative. Absolute refers to a decreased red cell mass and relative as a higher plasma volume. Absolute anemia fall into two major pathophysiologic categories: impaired cell production and increased cell destruction and loss in excess in which the bone marrow can't replace these loses. The presence of anemia maybe a bad sign of an underlying condition in which such identification is important to correct it. Relative anemia in which the plasma volume increasse can occur in pregnancy, macroglobulinemia and splenomegaly.
posted by luisbracero @ 11:12 PM
![]()
![]()

Optimistic,like changes,self-improvement,challenges,science,hardworker
